Edited by Brendan Striano, Grace Xiong, and Harry Lightsey - 7/1/2021
Most Common Fracture Types
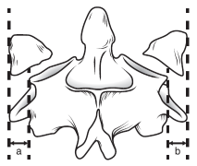
- Isolated Anterior Arch (Plough Fracture)
- Jefferson Fracture (Bilateral Ant. and Post. Arch Fracture)
- Unilateral Lat Mass Fracture
Exam Pearls
Ensure patient is in well-fitted C-Collar
Full BUE and BLE Neuro exam: Strength, Sensation, Reflexes, Hoffman, Babinski, Clonus, Rectal Tone +/- Bulbocavernosus, Tenderness to palpation; Spine Exam
- Good to get RN early because will need help with rolling pt for rectal / spine palpation
Workup
Radiographs: CT Cervical Spine (the majority of these consults will come having been diagnosed on CT)
Other imaging:
-if definitively non-operative, obtain upright (standing or sitting) XR Cervical Spine (AP + Lat) in ED or prior to discharge (for clinic comparison)
-MRI C-Spine (stat) if there is neurologic deficit warranting further investigation
-CT Angiogram Neck or MR Angiogram Neck - indicated if there is injury that extends into the Transverse Foramen (potential vertebral artery injury). If vertebral injury present, most pts asymptomatic, but good to know if pt is dependent on their remaining Vertebral Artery in the event pt needs surgery
Labs: Pre-op labs (in case injury is operative)
Other: Need to identify whether pt takes chronic anticoagulation; understand the remainder of patient’s trauma burden if applicable
Management
Need for acute intervention:
Yes, all C1 Fracture need immediate immobilization with C-collar
Some Fracture patterns can be definitively managed with C-collar
Acute neurologic compromise requires urgent surgical intervention
Injury Based Treatment Decision:
Plough Fracture
- Stable injury pattern treated with C-collar immobilization
Jefferson Fracture
- Conservative treatment with C-collar if stable pattern: ADI <3mm; Lat Overhang <7.8mm
- If unstable pattern, will likely need surgical intervention
-Unilateral Lateral Mass Fx_
- If stable pattern, Ok for C-collar
- If unstable, surgical intervention
Simply put, in the absence of neurologic compromise, safe to keep in a C-collar, pre-op pt, and keep NPO for AM discussion
Weight-bearing and range of motion: if managing definitively with C-collar, it should be maintained at all times
Type of immobilization: C-collar
Admission or discharge status: if definitively non-operative, OK to get XR Cervical spine in ED and discharge patient
Many of these injuries will occur in elderly geriatric patients who, even if fracture is safe for discharge, will need PT assessment, possible placement from ED or even admission
Anticoagulation: Does not need anticoagulation for this injury. If pt w/ c-spine injury needs anticoagulation for another reason (e.g. - risk of life or limb), need discussion between spine team and team desiring anticoagulation.
Factors to consider: need for surgical intervention for spine, likelihood to develop epidural hematoma because of injury v. risk of deterioration if not given anticoagulation
Antibiotics: None needed
Surgical Indications
Absolute:
Unstable C1 Injury
Atlanto-Dens Interval (ADI): >5mm = complete ligamentous disruption = unstable
Lateral Mass Overhang (via Open Mouth XR or (more likely) Coronal CT): > 7.8mm (collectively) is unstable
Neurologic Deficit requiring decompression
Relative: None
Not an indication: None