Edited by Grace Xiong, Harry Lightsey, Brendan Striano - 7/1/2021
Indications/Contraindications
Indications: Anterior hip dislocation (usually periprosthetic)
Contraindications: Fracture. It is important to scrutinize the initial XRs for fracture
Relative contraindications: Intraprosthetic dislocation, e.g. dislocated constrained liner (look for metal ring on x-ray), dislocated intraprosthetic dual mobility head (look for shadow of poly liner on the XR, and a head that seems “too small” for the shell).
Setup and Materials
Consent: It is important to explain to the patient that this is an attempt at a reduction and that failure may mean a trip to the operating room for a repeat closed reduction versus open reduction. Additionally, explain the low, but real risk of iatrogenic fracture or nerve injury
Materials:
Acquire immobilization (purple abduction pillow or knee immobilizer) prior to sedation so that it can be placed as soon as you finish without delay (don’t want to be scrambling once you’ve reduced a tenuous hip)
Sheet and/or second person to help prevent patient from falling off the bed.
Positioning:
Patient is supine on stretcher, at the edge of bed on the dislocated side.
Stretcher should be elevated as high as possible to allow for maximum hip extension.
Assistant is at the torso on the ipsilateral side to prevent patient from sliding off.
You are on the ipsilateral side of the dislocation at the hip/lower extremity.
Technique
Adequate sedation is critical for any successful reduction. The patient should be non-communicative to significant movement of the dislocated extremity. They should not be speaking, moving, attempting to grab you or others. If this is the case, work with your sedation team to increase sedation. Reduction attempts with inadequate sedation can lead to iatrogenic fracture and further injury.
Assess limb length prior to reduction - Important because sometimes restoration of length is the only sign of a successful reduction
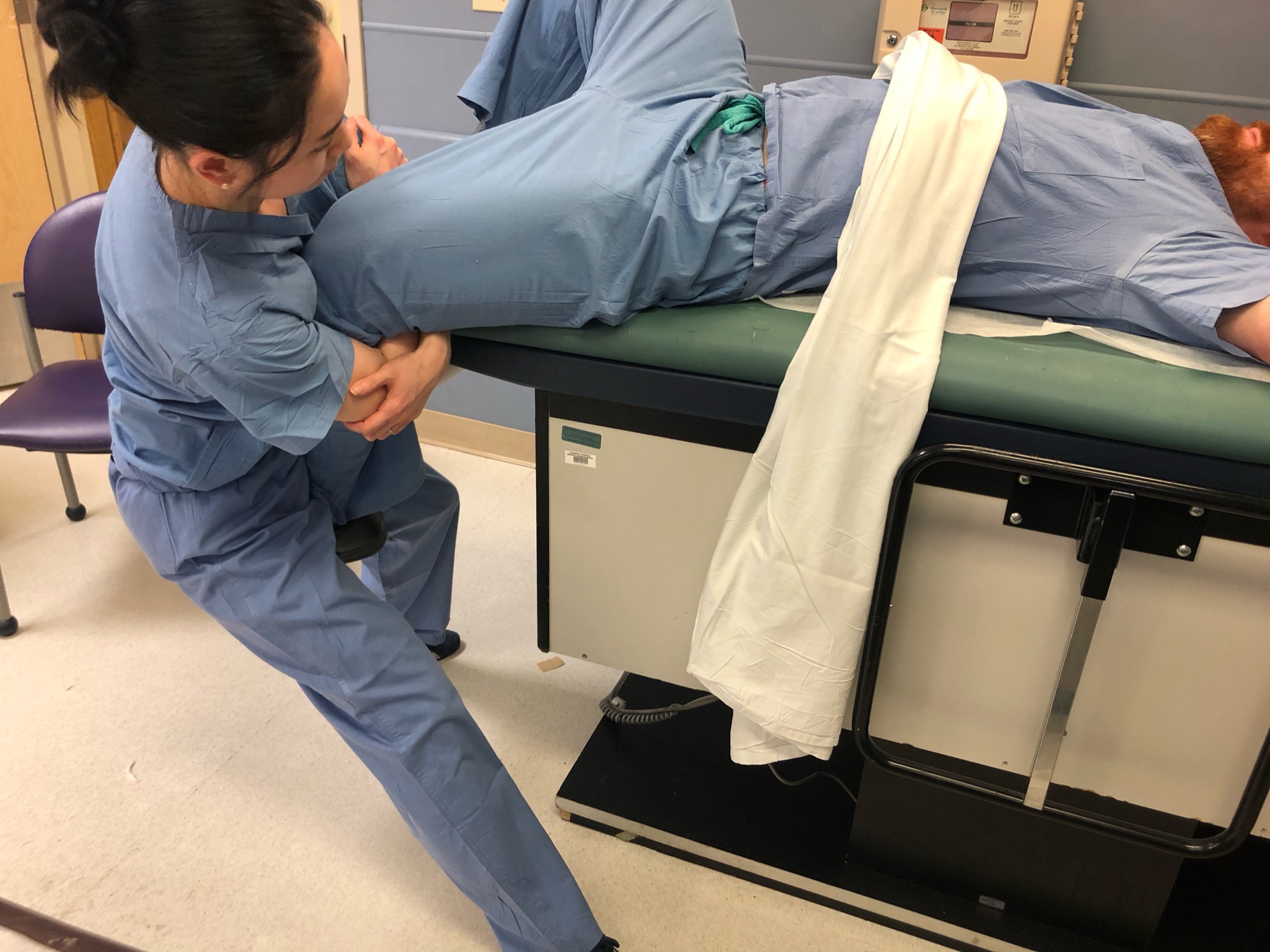
Bring the limb off the side of the bed to facilitate hip extension.
Flex the knee and use the lower leg as your guide for rotation.
Pull traction in extension and perform internal and external rotation to facilitate reduction.
External rotation:
Internal rotation:

Post reduction imaging and protocols
Imaging: Immediate portable AP to provisionally confirm reduction
Formal post-reduction AP and cross-table lateral XR of the hip
Immobilization: Knee immobilizer to prevent knee flexion (which in turns prevents hip flexion or extension).
Restrictions: WBAT bilateral lower extremities, no extension past neutral, no external rotation.
Follow up: 2 weeks with original surgeon.
Pearls & Pitfalls
Potential complications:
Femur fracture can occur if the patient is inadequately sedated and fighting reduction attempts.
Injury to the person performing the sedation is a real risk - remember to push and pull traction with your legs, not your back.
Tips for efficiency: Have the setup and materials (including sheets and assistants) before sedation begins. If you are working with an untrained assistant, you must give them specific instructions (which includes things like, don’t allow the patient to fall off the bed).