Edited by Grace Xiong, Harry Lightsey, Brendan Striano - 7/1/2021
Indications/Contraindications
Indications: Distal radius fracture
Contraindications: Ipsilateral injury (e.g. humerus or forearm fracture)
Technique
Preparation:
Perform your hematoma block first to allow local anesthetic time to take effect while you gather materials.
Materials:
Splint - dorsal volar splint if isolated distal radius fracture
Splint - sugar tong splint if rotationally unstable (e.g. large associated ulnar fragment). Beware of immobilizing the elbow in the elderly.
Two kerlix rolls or finger traps
Weights for hanging (can be IV bags or formal weights)
IV pole
Positioning:
Patient is upright or supine in stretcher.
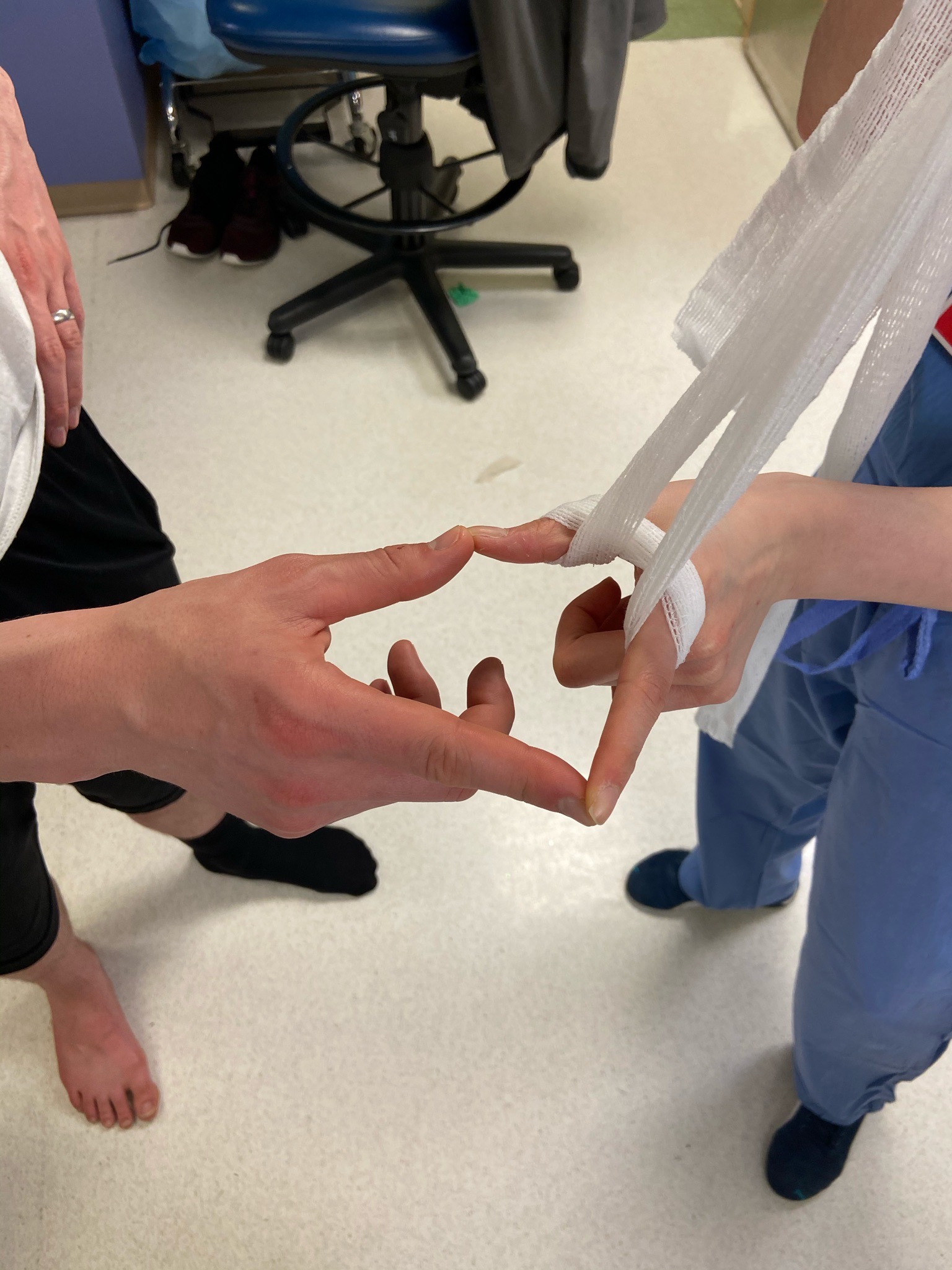
Suspend wrist via kerlix finger traps (see pictures below) to allow for ligamentotaxis to reduce/lengthen the fracture as the patient relaxes.

Place weights over the elbow to increase traction.

Technique:
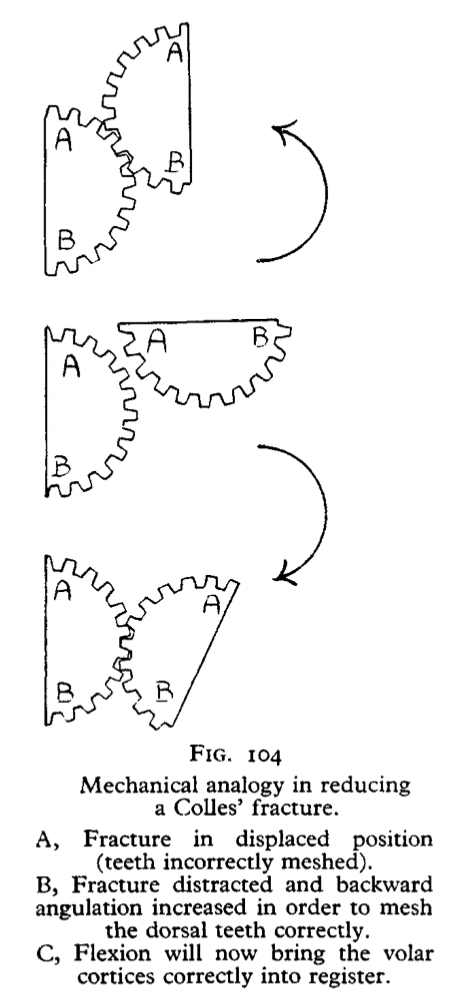
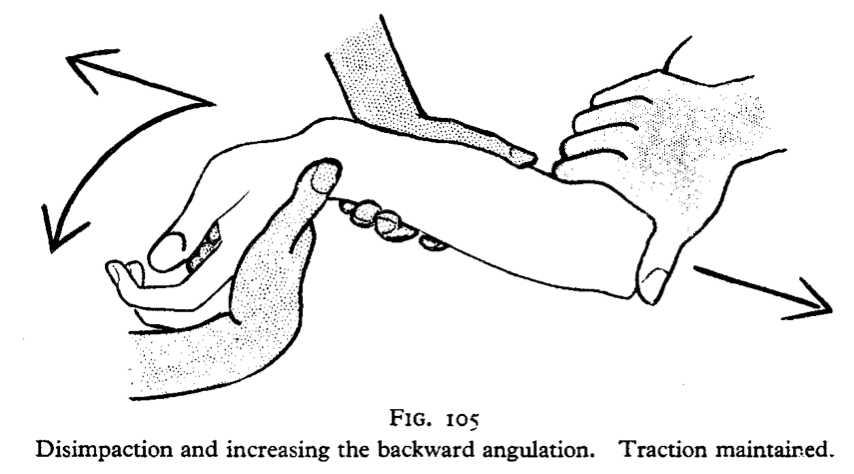
Key is to unhook the fracture by recreating the deformity prior to reducing the fracture.
One hand on the patient's hand, one on the forearm.
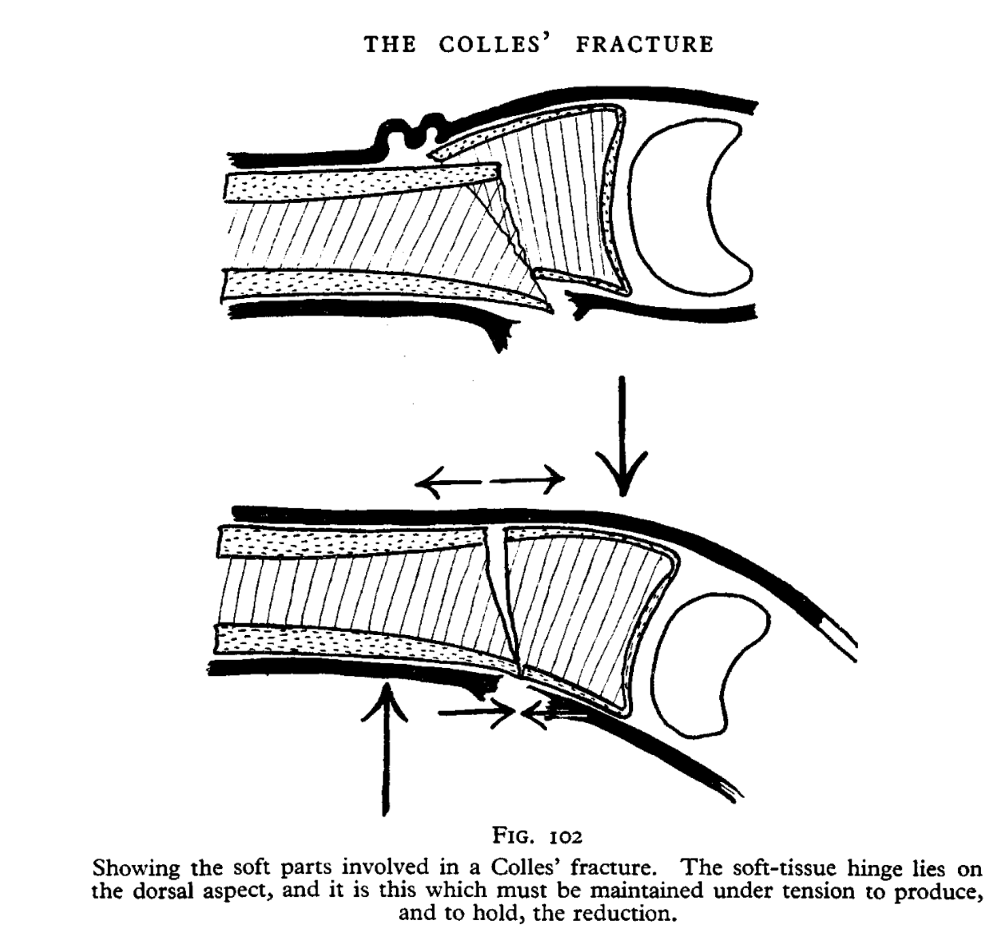
Three point mold on the splint.
Options for molding
Number 1: Mold with thumbs applying direct pressure

Number 2: Mold with two hands and knee

Number 3: Mold with fracture over the knee

Post reduction imaging and protocols
Imaging: Post-reduction AP and lateral films of the wrist
Immobilization:
Splint - dorsal volar splint if isolated distal radius fracture
Splint - sugar tong splint if rotationally unstable (e.g. large associated ulnar fragment). Beware of immobilizing the elbow in the elderly.
Restrictions: NWB upper extremity, encourage ROM at digits / shoulder
Follow up: 2 weeks ortho trauma, sports clinic, or upper extremity clinic
Pearls & Pitfalls
Potential complications:
Beware of excessive traction through associated radius and ulnar fractures as you may cause neurapraxia through the median nerve.
Tips for efficiency:
Have your set up before you begin (e.g. if you plan to splint, take fluoroscopy, etc., have all this turned on, at the bedside, rolled out, water ready, etc before you perform the reduction).
References
Images above referenced from The Closed Treatment of Common Fractures. John Charnley, B.Sc., M.B., F.R.C.S. Edinburgh, McLagan and Cumming, Ltd.; Baltimore, The Williams and Wilkins Company, 1950. $7.00, The Journal of Bone & Joint Surgery: July 1951