Edited by Phil Grisdela and Matt Fury - 7/1/2021
Indications/Contraindications
Rule out septic arthritis - exam with painful short arc range of motion through flexion/extension, especially internal and external rotation of the humerus with no other motion at the shoulder joint.
Workup: Infectious source (immunocompromised? IVDU? Positive blood cultures?), XR of the shoulder to rule out fracture, dislocation, or neoplasm (Axillary or Grashey + Scap Y), WBC, ESR/CRP
Materials/positioning
18g spinal needle
Chlorhexidine/alcohol wipes
Red top
Purple top
Lab/specimen bag
10cc syringe
Technique
Draw out landmarks if helpful - aiming for 2-3cm inferior and 1-2cm medial from posterolateral acromion. Have one hand on the coracoid anteriorly, aiming from this start point to the front 18g spinal needle with stylet in, aim towards coracoid, can ballot the humeral head by moving your free hand to feel interval between back of the glenoid and the humeral head Once you feel pop through, take stylet out, attach syringe and draw back
Anterior

Image borrowed from https://boneandspine.com/wp-content/uploads/2017/06/shoulder-aspration-anterior-300x258.png
Posterior
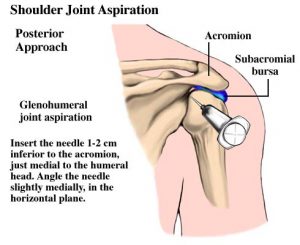
Image borrowed from https://boneandspine.com/wp-content/uploads/2017/06/shoulder-aspration-posterior-300x245.jpg
Pearls & Pitfalls
This is a difficult tap to get in an awake patient, pain control makes a big difference, as well as counseling appropriately. Can also be done in IR suite if dry tap or patient refuses.
Put in orders for joint aspiration first (Stat gram stain and culture go in the red top, cell count, crystals go into the purple top), let nurse know so they can print out the labels while you nail the tap. Walk the tubes to the lab yourself.