Edited by Grace Xiong, Harry Lightsey, Brendan Striano - 7/1/2021
Indications/Contraindications
Rule out septic knee or periprosthetic infection.
Workup as standard: Infectious source, XR to rule out fracture or dislocation or evaluate for foreign body, WBC, ESR/CRP
Materials/positioning
Materials:
18g spinal needle
Chlorhexidine/alcohol wipes
Red top
Purple top
Lab/specimen bag
10cc syringe
Positioning:
Supine
Knee slightly flexed over pillow
Chuck under knee to catch blood/fluid
Technique
Prep the area with chlorhexidine
Gather and ready supplies (have lab top tubes cleaned), lab labels prepped
Palpate landmarks
Many techniques possible (including just going for the most obvious effusion), however a reliable portal is the superolateral portal. Remember that you will need to angle your needle deeper than you think to go under the patella.
Aspirate at least 10 cc of fluid if possible.
Withdraw the needle quickly and change needles.
Divide the aspirate between the red top tube (first) and the lavender tube (must be second due to anticoagulant in tube). BE CAREFUL that you don't allow the tube suction to "steal" all the sample!
Apply labels, place in bag, and walk to lab yourself.
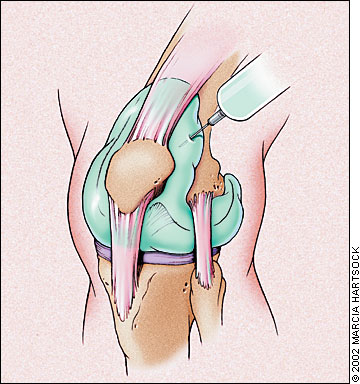
Image from https://www.aafp.org/afp/2002/1015/afp20021015p1497-f1.jpg
Pearls & Pitfalls
Make sure you look at XR first.
Inferomedial aspirations can yield fluid, but in native knees may be blocked by the fat pad.